Your heart is a strong muscular pump. It is responsible for pumping about 3,000 gallons of blood throughout your body every day. Like other muscles in your body, your heart itself needs to receive a good supply of blood at all times to function properly. Your heart muscle gets the blood it needs to do its job from your coronary arteries.
What is coronary artery disease?
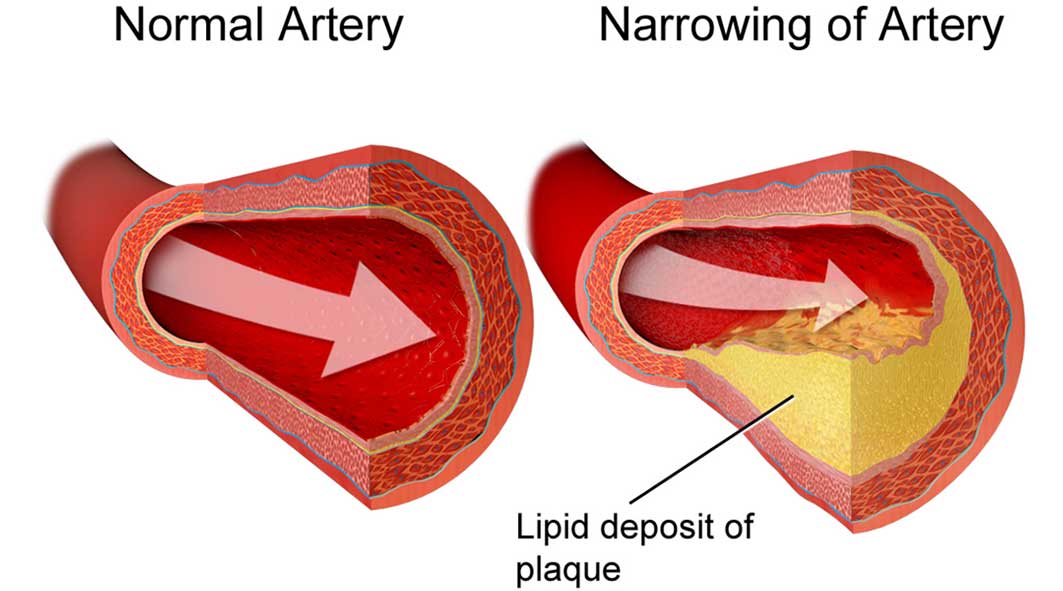
Coronary artery disease is the narrowing or blockage of the coronary arteries, usually caused by atherosclerosis. Atherosclerosis (sometimes called “hardening” or “clogging” of the arteries) is the buildup of cholesterol and fatty deposits (called plaques) on the inner walls of the arteries. These plaques can restrict blood flow to the heart muscle by physically clogging the artery or by causing abnormal artery tone and function.
Without an adequate blood supply, the heart becomes starved of oxygen and the vital nutrients it needs to work properly. This can cause chest pain called angina.
If the blood supply to a portion of the heart muscle is cut off entirely, or if the energy demands of the heart become much greater than its blood supply, a heart attack (injury to the heart muscle) may occur.
What causes the coronary arteries to narrow?
Your coronary arteries are shaped like hollow tubes through which blood can flow freely. The muscular walls of the coronary arteries are normally smooth and elastic and are lined with a layer of cells called the endothelium. The endothelium provides a physical barrier between the bloodstream and the coronary artery walls while regulating the function of the artery by releasing chemical signals in response to various stimuli.
Coronary artery disease starts when you are very young. Before your teen years, the blood vessel walls begin to show streaks of fat. As you get older, the fat builds up, causing slight injury to your blood vessel walls. Other substances traveling through your bloodstreams, such as inflammatory cells, cellular waste products, proteins, and calcium begin to stick to the vessel walls. The fat and other substances combine to form a material called plaque.
Over time, the inside of the arteries develop plaques of different sizes. Many of the plaque deposits are soft on the inside with a hard fibrous “cap” covering the outside. If the hard surface cracks or tears, the soft, fatty inside is exposed. Platelets (disc-shaped particles in the blood that aid clotting) come to the area, and blood clots form around the plaque. The endothelium can also become irritated and fail to function properly, causing the muscular artery to squeeze at inappropriate times. This causes the artery to narrow even more.
Sometimes, the blood clot breaks apart, and the blood supply is restored. In other cases, the blood clot (coronary thrombus) may suddenly block the blood supply to the heart muscle (coronary occlusion), causing one of three serious conditions, called acute coronary syndromes.
What are acute coronary syndromes?
Unstable angina: This may be a new symptom or a change from stable angina. Angina may occur more frequently, occur more easily at rest, feel more severe, or last longer. Although this can often be relieved with oral medications, it is unstable and may progress to a heart attack. Usually more intense medical treatment or a procedure is required to treat unstable angina.
Non-ST segment elevation myocardial infarction (NSTEMI): This type of heart attack, or MI, does not cause major changes on an electrocardiogram (ECG). However, chemical markers in the blood indicate that damage has occurred to the heart muscle. In NSTEMI, the blockage may be partial or temporary, so the extent of the damage is relatively minimal.
ST-segment elevation myocardial infarction (STEMI): This type of heart attack, or MI, is caused by a prolonged period of blocked blood supply. It affects a large area of the heart muscle, and causes changes on the ECG as well as in blood levels of key chemical markers.
Some people have symptoms that indicate they may soon develop the acute coronary syndrome, others may have no symptoms until something happens, and still, others have no symptoms of acute coronary syndrome at all.
All acute coronary syndromes require emergency evaluation and treatment.
Collateral Circulation
As the size of the blockage in a coronary artery increases, the narrowed coronary artery may develop “collateral circulation.” Collateral circulation is the development of new blood vessels that reroute blood flow around the blockage. However, during times of increased exertion or stress, the new arteries may not be able to supply enough oxygen-rich blood to the heart muscle.
What is ischemia?
Ischemia is a condition described as “cramping of the heart muscle.” Ischemia occurs when the narrowed coronary artery reaches a point where it cannot supply enough oxygen-rich blood to meet the heart’s needs. The heart muscle becomes “starved” for oxygen.
Ischemia of the heart can be compared to a cramp in the leg. When someone exercises for a very long time, the muscles in the legs cramp up because they’re starved for oxygen and nutrients. Your heart, also a muscle, needs oxygen and nutrients to keep working. If the heart muscle’s blood supply is inadequate to meet its needs, ischemia occurs, and you may feel chest pain or other symptoms.
Ischemia is most likely to occur when the heart demands extra oxygen. This is most common during:
* Exertion (activity)
* Eating
* Excitement or stress
* Exposure to cold
When ischemia is relieved in less than 10 minutes with rest or medications, you may be told you have “stable coronary artery disease” or “stable angina.” Coronary artery disease can progress to a point where ischemia occurs even at rest.
Ischemia, and even a heart attack, can occur without any warning signs and is called “silent” ischemia. Silent ischemia can occur among all people with heart disease, though it is more common among people with diabetes.
What are the symptoms of coronary artery disease?
The most common symptom of coronary artery disease is angina (also called angina pectoris). Angina is often referred to as chest pain. It is also described as chest discomfort, heaviness, tightness, pressure, aching, burning, numbness, fullness, or squeezing. It can be mistaken for indigestion or heartburn. Angina is usually felt in the chest, but may also be felt in the left shoulder, arms, neck, back or jaw.
Other symptoms that can occur with coronary artery disease include:
* Shortness of breath
* Palpitations (irregular heartbeats, skipped beats or a “flip-flop” feeling in your chest)
* A faster heartbeat
* Dizziness
* Nausea
* Extreme weakness
* Sweating
If you experience any of these symptoms, it is important to call your doctor, especially if these are new symptoms or if they have become more frequent or severe.
Symptoms in Women
Women often have different symptoms of coronary artery disease than men. For example, symptoms of a heart attack in women include:
* Pain or discomfort in the chest, left arm or back
* Unusually rapid heartbeat
* Shortness of breath
* Nausea or fatigue
What you should do if you have symptoms:
If you have not been diagnosed with coronary artery disease and any of these symptoms occur, it is important to get medical help right away – call 9-1-1 or have someone take you to the nearest emergency room.
If you have been prescribed nitroglycerin and experience angina, stop what you are doing and rest. Take one nitroglycerin tablet and let it dissolve under your tongue, or if using the spray form, spray it under your tongue. Wait 5 minutes. If you still have angina after 5 minutes, call 911 to get emergency help.
For patients diagnosed with chronic stable angina: If you experience angina, take one nitroglycerin tablet and let it dissolve under your tongue, repeating every 5 minutes for up to 3 tablets spanning 15 minutes. If you still have angina after taking 3 doses of nitroglycerin, call 911 to get emergency help.
Use of Aspirin with unstable chest pain: After you call 9-1-1, if you do not have a history of aspirin allergy or bleeding, emergency personnel may advise that you chew one full (325 mg) aspirin slowly. It’s especially effective if taken within 30 minutes of the onset of symptoms.
Do not drive yourself to the hospital. In many cases, the emergency personnel can begin to give you heart-saving care right away.
To prevent damage to your heart muscle, do not delay seeking medical treatment.
SPECIAL NOTE:
Some people worry that they shouldn’t call 9-1-1 because they think their symptoms will subside or they are embarrassed. However, it’s better to have your symptoms evaluated as soon as possible so you can receive quick treatment in the event of a heart attack.
How is coronary artery disease diagnosed?
Your doctor diagnoses coronary artery disease by talking to you about your symptoms, reviewing your medical history and risk factors, and performing a physical exam.
Diagnostic tests, including blood tests, an electrocardiogram (ECG or EKG), exercise stress tests, cardiac catheterization, and others may be required to appropriately diagnose and treat coronary artery disease. These tests help your doctor evaluate the extent of your coronary heart disease, its effect on the function of your heart, and the best form of treatment for you.
Research into new testing procedures, such as coronary computed tomography angiogram (CTA), may change the way coronary artery disease is diagnosed in the future.
What are the risk factors for coronary artery disease?
Non-modifiable risk factors (those that cannot be changed) include:
* Male gender. The risk of heart attack is greater in men than in women, and men have heart attacks earlier in life than women. However, at age 70 and beyond, men and women are equally at risk.
* Advanced age. Coronary artery disease is more likely to occur as you get older, especially after age 65.
* Family history of heart disease. If your parents have heart disease (especially if they were diagnosed with heart disease before age 50), you have an increased risk of developing it.
Ask your doctor when it’s appropriate for you to start screenings for heart disease so it can be detected and treated early.
* Race. African Americans have more severe high blood pressure than Caucasians and therefore have a higher risk of heart disease. Heart disease risk is also higher among Mexican Americans, American Indians, native Hawaiians, and some Asian Americans. This is partly due to higher rates of obesity and diabetes in these populations.
Modifiable risk factors (those you can treat or control) include:
* Cigarette smoking and exposure to tobacco smoke
* High blood cholesterol and high triglycerides — especially high LDL or “bad” cholesterol over 100 mg/dL and low HDL or “good” cholesterol under 40 mg/dL. Some patients who have existing heart or blood vessel disease and other patients who have a very high risk should aim for an LDL level less than 70 mg/dL. Your doctor can provide specific guidelines.
* High blood pressure (140/90 mm/Hg or higher)
* Uncontrolled diabetes
* Physical inactivity
* Being overweight (body mass index or BMI from 25-29 kg/m2) or being obese (BMI higher than 30 kg/m2)
NOTE:
How your weight is distributed is important. Your waist measurement is one way to determine fat distribution. Your waist circumference is the measurement of your waist, just above your navel. The risk of cardiovascular disease increases with a waist measurement of over 35 inches in women and over 40 inches in men.
* Uncontrolled stress or anger
* Diet high in saturated fat and cholesterol
* Drinking too much alcohol
The more risk factors you have, the greater your risk of developing coronary artery disease.
How is coronary artery disease treated?
Treatment for coronary artery disease involves reducing your risk factors, taking medications, possibly undergoing invasive and/or surgical procedures and seeing your doctor for regular visits. Treating coronary artery disease is important to reduce your risk of heart attack or stroke.
Reduce your risk factors
Reducing your risk factors involves making lifestyle changes. Your doctor will work with you to help you make these changes.
* If you smoke, you should quit.
* Make changes in your diet to reduce your cholesterol, control your blood pressure, and manage blood sugar if you have diabetes. Low fat, low sodium, low cholesterol foods are recommended. Limiting alcohol to no more than one drink a day is also important. A registered dietitian can help you make the right dietary changes. Cleveland Clinic offers nutrition programs and classes to help you reach your goals.
* Increase your exercise/activity level to help achieve and maintain a healthy weight and reduce stress. But, check with your doctor before starting an exercise program. Ask your doctor about participating in a cardiac rehabilitation program.
Test your 10-year risk for heart attack.
Take Medications As Prescribed
If lifestyle changes aren’t enough to control your heart disease, medications may be prescribed to treat certain risk factors, such as high cholesterol or high blood pressure. The medications prescribed will depend on your personal needs, the presence of other health conditions, and your specific heart condition.
Have Procedures to Treat Coronary Artery Disease, as Recommended
Interventional procedures
Common interventional procedures to treat coronary artery disease include balloon angioplasty (PTCA) and stent or drug-eluting stent placement. These procedures are considered non-surgical because they are done by a cardiologist through a tube or catheter inserted into a blood vessel, rather than by a surgeon through an incision. Several types of balloons and/or catheters are available to treat the plaque within the vessel wall. The physician chooses the type of procedure based on individual patient needs.
Coronary artery bypass graft (CABG) surgery
One or more blocked coronary arteries are bypassed by a blood vessel graft to restore normal blood flow to the heart. These grafts usually come from the patient’s own arteries and veins located in the chest, leg, or arm. The graft goes around the clogged artery (or arteries) to create new pathways for oxygen-rich blood to flow to the heart.
When these traditional treatments are not an option, doctors may suggest other less traditional therapies, such as TMR or EEC.
Transmyocardial laser revascularization (TMR)
TMR is a treatment aimed at improving blood flow to areas of the heart that were not treated by angioplasty or surgery. A special carbon dioxide (CO2) laser is used to create small channels in the heart muscle, improving blood flow in the heart. Frequently, it is performed with coronary artery bypass, occasionally alone.
For patients who have persistent angina symptoms and have exhausted the standard treatments without successful results, Enhanced External Counterpulsation (EECP) may stimulate the openings or formation of collaterals (small branches of blood vessels) to create a natural bypass around narrowed or blocked arteries. EECP is a non-invasive treatment for people who have chronic, stable angina; who are not receiving adequate relief from angina by taking nitrate medications; and who do not qualify for an invasive procedure such as bypass surgery, angioplasty or stenting.
For patients who have persistent angina symptoms and have exhausted the standard treatments without successful results, Enhanced External Counterpulsation (EECP) may stimulate the openings or formation of collaterals (small branches of blood vessels) to create a natural bypass around narrowed or blocked arteries. EECP is a non-invasive treatment for people who have chronic, stable angina; who are not receiving adequate relief from angina by taking nitrate medications; and who do not qualify for an invasive procedure such as bypass surgery, angioplasty or stenting.
Important Note: These procedures increase blood supply to your heart, but they do not cure coronary heart disease. You will still need to decrease your risk factors by making lifestyle changes, taking medications as prescribed and following your doctor’s recommendations to prevent future disease.
The Miller Family Heart & Vascular Institute cardiologists and surgeons specialize in the treatment of coronary artery disease. The team approach at the Miller Family Heart & Vascular Institute at Cleveland Clinic ensures that patients receive the best care before, during, and after their procedure.
Your cardiologist (heart doctor) will want to see you on a regular basis for a physical exam and possibly to perform diagnostic tests. Your doctor will use the information gained from these visits to monitor the progress of your treatment. Check with your heart doctor to find out when to schedule your next appointment.



